
The Digital Efficiency Dividend
Digital health platforms can be a significant investment for any healthcare provider.
In this whitepaper series, we investigate the return on that investment. This edition identifies key areas of waste and how investing in digital health in those areas can improve efficiency and reduce patient length of stay.
Executive Summary
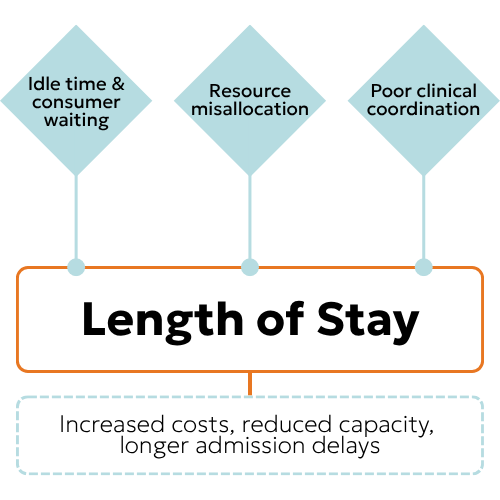
These sources of hospital inefficiency can be addressed with digital health solutions, reducing consumer Length of Stay.
Systemic communication gaps between departments drive bed congestion and idle time across hospitals. An integrated platform enables real‑time coordination and predictive resource allocation, reducing assessment delays and length of stay. As demonstrated in emergency and surgical settings, door‑to‑intervention times can be halved, and patient flow can be improved without replacing existing systems.
Inappropriate testing, manual logistics, and rigid scheduling waste resources hospital‑wide. Mobile applications and interoperable health information technology enable real‑time access to accurate data, reducing errors and decision delays. As shown in pathology, radiology, and transfer processes, this lowers costs, shortens throughput time by over 12%, and reduces readmissions.
Poor care coordination contributes to most adverse events, with staff frequently unable to reach colleagues. A single integration engine connects any system to any person, enabling standardised best practice across wards and hospitals. Real‑time information sharing and automated tracking reduce intervention times from hours to minutes, shorten stays, and improve clinical outcomes.
Overall hospital efficiency is often measured by average length of stay, and improved service delivery and productivity reduce admission time, directly benefiting bed capacity and costs, with digital health implementations saving as much as 20% on length of stay.
Inefficiency in healthcare systems.
Government healthcare expenditure equates to around 10% of Gross Domestic Product (GDP) (1). Even with that level of investment, ambulance ramping remains a concern across all Australian jurisdictions, with levels increasing in each period leading into 2025 (2).
There are two obvious approaches to improving the capacity of any system, public healthcare included:
- Increasing the resources available, or
- Improving the efficiency of using existing resources.
While increased investment is always a matter for public discourse, as a health tech company, Ikonix Technology is interested in investigating how our current and future customers can utilise technology to drive efficiency in healthcare delivery.
In doing so, we can identify a few areas where inefficiencies may exist and then apply a digital health solution to address them. From there, we can work towards quantifying the opportunity healthcare providers may be able to access through their investment in digital health platforms.
One literature review identifies several categories of areas where different healthcare organisations may experience inefficiencies:
- Transportation – unnecessary movement of patients and staff
- Motion – physical movement that isn’t in aid of actual productive work, such as searching for equipment, drugs and paperwork
- Inventory – financing and storage expenses, and patients waiting, particularly where there is scarcity
- Waiting – idle time such as waiting for results, staff or medicines, or by scheduling errors
- Over-production – Producing more than the required, or before or without a need, such as unnecessary diagnostics
- Over-processing – unintentionally doing more processing work than required, including unnecessarily repeating tests or reconfirming data
- Defects – this might include paperwork errors, incorrect work, generating waste, and readmission after failed discharge (3)
We can group these into three clear themes of inefficiency:
- Idle time and customer waiting,
- Allocation and utilisation of assets, and
- Coordination of clinical labour.
In this article, we’ll examine each of these and how improvements in any or all of them lead to improvements in one of the key metrics of hospital efficiency: Length of Stay. This is the consumer’s time spent between admission and discharge, often measured as an average.
Improvements in ALOS can confirm the ultimate success of any digital health solution in improving hospital efficiency.
Patient wait times before and after admission
Section Summary
- Congestion and slow throughput delay patients’ access to services (triage to treatment), reduce the capacity of service delivery in diagnostics and treatment, and keep dischargeable patients in needed beds longer than necessary. Collectively, we are describing this as idle time.
- Digital health solutions can reduce communication gaps, automate workflows, and reduce the possible points of failure, reducing this idle time.
- Improvements can be quantified using standard wait-time metrics, such as time between presentation and triage, triage and being seen by a clinician, as well as condition-specific metrics, such as the example door-to-balloon or ECG times.
Patient idle times for treatment and admission have increased across metropolitan acute public hospitals. The variation in length of stay among admitted patients has a consequential effect on access to hospital beds for those waiting in the emergency department (4). When the hospital becomes congested, idle time at admission increases, reducing the ability to place incoming patients in the required beds.
In a study that included one Berlin hospital, the average triage time during peak hours was 48 minutes, with 33% of cases exceeding the 15‑minute benchmark for initial assessment. Admission processing averaged 3.6 hours, particularly for internal medicine and geriatrics, while discharge took between 1.8 and 2.2 hours.
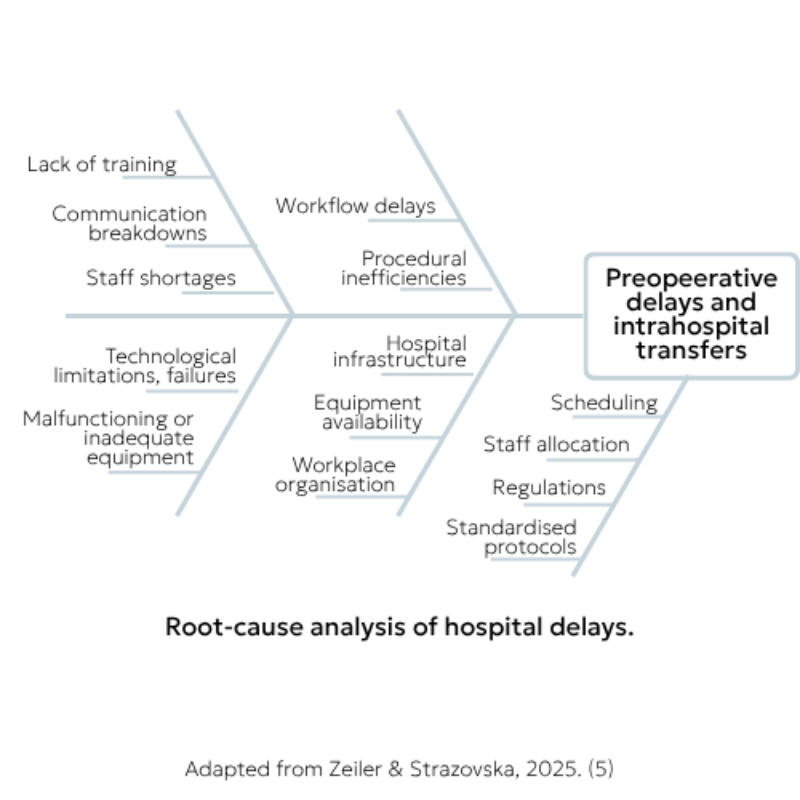
The authors attributed this to poor communication between departments being the primary driver of patient waiting:
- Interviews with six ED physicians identified systemic communication gaps between the emergency department and inpatient services as the primary cause of delayed transfers.
- Inefficiencies in patient transfer processes, including poor bed tracking and handovers, resulted in internal delays.
- Delays in radiology were linked to equipment downtime and prioritisation of emergency cases, while outpatient clinics faced delays due to misalignment with inpatient discharges and emergency department retention. (5)

A variety of studies have identified methods relevant to specific health concerns and hospital processes that can improve the efficiency of care services. There are many procedures conducted in hospitals, and we can only select clear examples to illustrate the possibilities for applying digital health solutions in this context.
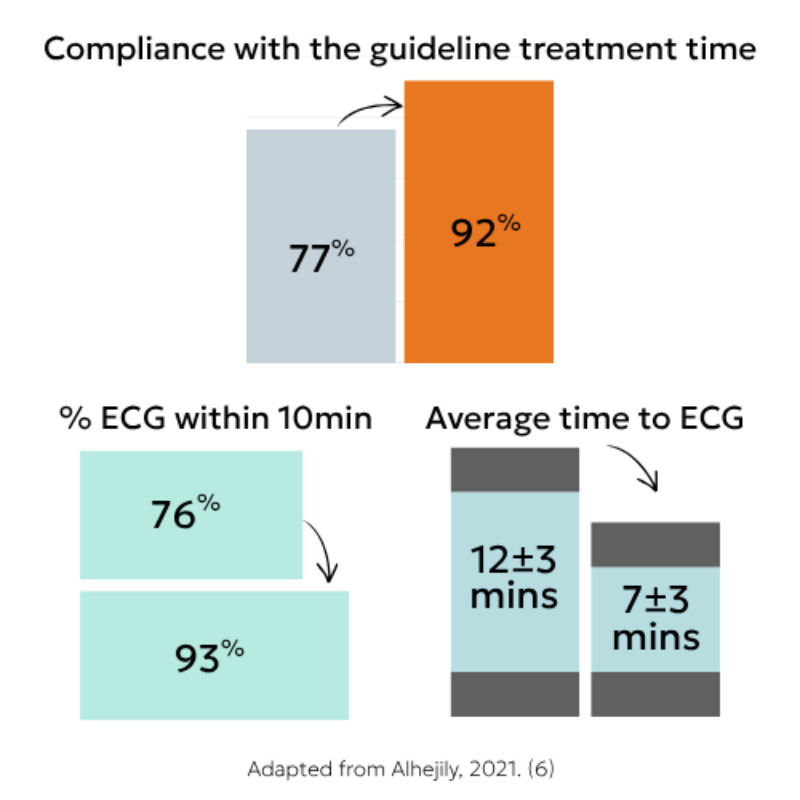
In a study of ED presentations with chest pain, implementing a continuous improvement protocol that used the group messaging features of a consumer-grade app to provide instantaneous feedback on suspected acute coronary syndrome (ACS) yielded measurable results. Cases were posted on the group once activation was made, timelines were provided, and team leaders commented. Weekly assessments ensured compliance and highlighted areas for improvement. After six months of the improvement program, door‑to‑balloon time improved from 77% to 92%. Door‑to‑ECG time was reduced from 12 ± 3 minutes in the first quarter to 7 ± 3 minutes in the last quarter, with 93% compliance with guideline timeframes, compared with 76% before the program (6).
Information technology infrastructure is a critical success factor for wait reduction. At a network level and supported by appropriate digital health solutions to integrate the technologies, centralised queue waiting lists (single-entry models, pooled waiting lists, equalisation between providers) have consistent evidence of effectiveness in reducing waitlists and promoting utility and equity, including reduced waitlist mortality and improved post-surgery survival. Further, the Agency for Clinical Innovation at NSW Health suggests decentralised surgical care, in which tertiary hospitals transfer low-acuity patients to community hospitals. They identify IT infrastructure as a key facilitator of success, along with physician and patient engagement, team‑based cooperative care, and ongoing evaluation (7)

Quantifying the improvement is possible using standard wait-time metrics and operational KPIs. An important metric is the time a person waits to be seen by a clinician after triage (4). Additional quantifiable measures include triage times, admission processing time, and discharge duration. These can be enhanced with condition-specific metrics, such as door-to-balloon time and door-to-ECG time. Each of these can be monitored and reported through integrations with the Electronic Medical Record, enabling hospital personnel to update the Record in near real time (6).
Longitudinally, these can also be evidenced in Average Length of Stay and Average Bed Occupancy rates. Reduced length of stay is a quantifiable return from improved patient flow. In the same ACS study, early invasive strategy and case detection reduced the median admission time from 4 days to 2.5 days.

Resource allocation and utilisation.
Section Summary
- Inappropriate, repeated and otherwise unnecessary service and facility use, as well as errors in documentation antecedent to these, result in hospital inefficiencies.
- Mobile applications, system interoperability, automated or enhanced workflow, and leveraging real‑time data and predictive tools can help to improve resource use measurably.
- The resulting improvement in asset and personnel utilisation reduces delays caused by unnecessary initial or confirmatory tests, such as almost one-third of some pathology tests being unnecessary, or direct increase of the total number of MRI exams one facility was able to conduct, without any change in staffing or equipment.
The Institute for Healthcare Improvement explains that inappropriate use of clinical services wastes resources without improving outcomes. The systematic use of more (or fewer) resources than necessary, including CT or MRI instead of an X-ray, unnecessary admission, and inappropriate antibiotic use, all represent a direct drain on health system sustainability (9). Where a service such as an MRI is unnecessarily reserved or misapplied, it’s also less available to those who more appropriately need that service, further adding to the idle times discussed above.
In a sample of 7074 urine microscopy, culture, and sensitivity requests (88 per 1000 ED presentations), an estimated 27% of tests could have been safely avoided given the absence of clinical symptoms. Nearly half (41.6%) of patients were treated with antibiotics, and 22.4% were treated without a positive test result (9). This means both the impact of overprescribing on the patient and the unnecessary consumption of hospital materials.
The absence of IT tools to support internal transportation processes, in which medicine location events were not recorded electronically, meant that in one study, locating missing items required multiple staff members to manually review paper records, making the process time-consuming and inefficient (10).
Mobile technologies can reduce errors and accelerate decision‑making in real time. Implementing mobile applications enables medical personnel to access accurate, up‑to‑date information immediately, reducing decision-making delays. Electronic input, retrieval, and updating of information minimises risks such as miscommunication, lost paperwork, and delays in updating critical data. This improvement in accuracy accelerates logistical operations and ensures that medical teams have the right information at the right time (10).
At a higher, systemic level, health information technology interoperability shortens transfer times and reduces readmissions. HIT interoperability during interhospital transfer reduced throughput time by 45.6 minutes (12.0%) on average. When interoperability was enabled through a common HIE vendor, the reduction was 15.6% greater than when different vendors were used. Furthermore, interoperability led to a 3% decrease in the 30-day all-cause readmission rate among transferred patients, demonstrating a significant positive impact on patient outcomes. (11)
Operating room efficiency can be improved through scheduling strategies and enabling technologies. Strategies with consistent positive evidence include separating emergent from planned surgery; high-volume, low-complexity lists; block schedules; split blocks; open blocks for add-on cases; the golden patient approach (the most medically fit patient first); and scheduling patients requiring inpatient beds postoperatively as late in the block as possible. Enablers include performance monitoring, staff feedback and education, team briefings and morning huddles, quality improvement cycles (PDCA, Lean, Six Sigma), standard operating procedures, checklists, data‑driven caseload prediction, and artificial intelligence (machine- and deep-learning models). (7)
Real‑time cancellation notification and ICT integration can increase daily examination capacity. Previously, MRI cancellation notifications stopped at the hospital reception desk, and the radiology department could not capture them, meaning vacant slots could not be used effectively. By mandating that reception contacts the examination room directly upon cancellation, waiting patients could be brought forward and emergency examinations accommodated, increasing the number of daily examinations by approximately five (12)
Quantifying the improvement in resource allocation uses cost savings, time reductions, throughput increases, and outcome measures. Specific quantifiable metrics drawn from the evidence include: avoided service cost savings (e.g., $39,538 from avoided MCS tests)(9), mobility throughput time reduction (45.6 minutes or 12% per transfer)(11), readmission rate reduction (3.0 percentage points)(6), daily examination increase (approximately five additional MRI scans)(12), and length of stay reductions. Each of these can be measured before and after the implementation of digital health to demonstrate return on investment.
Electronic bed management and just‑in‑time bed assignment are emerging strategies. The Agency for Clinical Innovation found early but promising evidence supporting electronic bed management systems and just-in-time bed assignment. This involves assigning ready beds to patients ready to move rather than preassigning them. Enhanced digital infrastructure for real‑time bed vacancy prediction and management can help increase postoperative recovery capacity (7).
Coordination of care delivery.
Section Summary
- Poor care coordination creates delays, duplication, and communication failures that waste resources and harm patients. Clinicians often find it difficult to access the right people at the right time.
- Better and automated information sharing saves time and reduces variability, reducing the length of time patients must remain admitted to the hospital.
- Various studies have shown improved coordination resulting in faster critical procedure occurrence, such as from stroke identification to thrombolysis, STEMI ED presentation to ECG and balloon time, and more. All of which reduce patient Length of Stay.
Poor care coordination creates delays, duplication, and communication failures that waste resources and harm patients. The Institute for Healthcare Improvement identifies inefficiencies in flow, throughput, communication, and coordination as direct sources of waste, including delayed laboratory results, readmissions, longer-than-expected length of stay, beds held for admission or transfer, and artificial variability due to lack of coordination. (8)
Specific coordination failures cascade across disciplines, prolonging patient stay and duplicating work. In a study of emergency department–psychiatry patient flow, delays included: on‑call psychiatry doctors receiving delayed handover from ED staff; ED nursing receiving delayed handover from psychiatry; social work reporting prolonged stays due to delayed referrals from ED and psychiatry; and failure to assess patients in tandem across disciplines. Duplication included both the ED nurse and the triage nurse separately phoning psychiatry doctors about the same patient, and overlapping assessments between social work and psychiatry. Communication difficulties included psychiatry failing to update ED nurses on management plans, ED staff being hard to identify for updates, security not being updated (lengthening security interventions), and delayed updates to healthcare assistants (lengthening 1:1 special observations). (14)

Poor communication is a leading cause of harm, contributing to 70% of adverse events and identified as the root cause in 65% of sentinel patient events. Many clinical communications are ad hoc, inter‑team and role‑based, making practice overly complex and highly variable. Front‑line clinicians struggle to identify who is performing a specific clinical role at any given time. Multiple different communication methods exist, and individual receiver preferences dictate which method is used – preferences that Switchboard may know but are not generally visible to clinical staff. (13)
Nearly half of clinicians cannot contact relevant staff on the first attempt more than half the time. Fifty‑five of 115 respondents in one study at an Australian healthcare facility (47.8%) reported being unable to contact someone on the first attempt more than half the time. This drives continued reliance on switchboard services, which have access to accurate staffing rosters and can redirect calls. The cognitive and emotional stresses of interruptions are well documented, and when multiple communication modalities operate simultaneously (e.g., SMS interrupting phone calls), complexity increases further. (13)

Digital health solutions enable standardised, centralised coordination with real‑time information sharing. Organised, centralised systems with multidisciplinary team membership are considered optimal for diagnostic cancer assessment services. Reducing a pathway by one day early may save multiple days later, particularly when tests are scheduled as soon as required. (15) Even across hospitals, standardisation reduces the average length of stay. Integration and communication tools enable the standardisation of best practice within and across hospitals.
Standardised, multidisciplinary approaches using EHR‑integrated clinical decision support reduce clinical variation across hospitals. In response to significant intersite and temporal variability in the incidence of postoperative acute kidney injury (PO-AKI), a quality improvement initiative implemented risk assessment models, practice alerts, and order sets, along with mitigation care bundles, across a regional healthcare system. The initiative demonstrated that standardised approaches leveraging EHR‑integrated CDS and improvement science can meaningfully reduce clinical variation across multiple surgical service lines. (16)
Real‑time information sharing and automated time tracking dramatically improve stroke care coordination. Following implementation of an in‑hospital stroke system with real‑time information sharing (pre‑notifications to team members and efficient multidisciplinary communication) supported by digital clinical collaboration tools, door‑to‑needle time decreased from 118 minutes to 26 minutes. The proportion of patients receiving intravenous thrombolysis within 60 minutes increased from 17.39% to 92.64%. Hospital stays shortened from 10 days to 8 days, and NIHSS scores at discharge improved significantly. Gaps that prolonged door‑to‑needle time were easily identified, enabling continuous quality improvement. (17)
Care coordination technology enables easier access to service providers, better communication between stakeholders, sharing of patient information, and more complete records. Programmatic benefits have included significant reductions in psychological distress and patient needs related to daytime activity, company, physical health, employment, and access to other services. For guardians of adults with severe mental illness, care coordination delivered significant decreases in psychiatric hospitalisations, days admitted in psychiatric hospital, emergency room visits, arrests, and costs per consumer. (18)

Quantifying the improvement in care coordination uses time metrics, clinical outcomes, readmissions, and cost reductions. Specific quantifiable measures from the evidence include: door‑to‑needle time (from 118 to 26 minutes), thrombolysis within 60 minutes (17% to 93%), length of stay (10 to 8 days)(17), NIHSS score improvement, psychiatric hospitalisation rates and days admitted, emergency room visits, arrests, costs per consumer, and reduction in clinical variation across sites (18). Each can be tracked before and after the implementation of coordinated digital health systems to demonstrate return on investment.
The Wound Care Command Centre is a digital-first clinical initiative of the Sydney Local Health District that has reduced ALOS. In a study by the Centre, researchers examining length of stay found that this care model significantly reduced the time chronic wound patients spent in the hospital (20). A specialised, coordinated team of nurses was able to provide immediate patient advice, which in turn improved patient outcomes and delivered ‘substantial cost savings’.

The impact on Length of Stay.
- Overall hospital efficiency is frequently examined using a patient’s Average Length of Stay.
- Improved service delivery and productivity reduces the time patients spend admitted, with a direct impact on capacity and cost.
- Different digital health implementations achieve these dividends, saving as much as 20% LOS
Length of stay (LOS) and its average (ALOS) measure the days a patient spends admitted to a hospital. This metric is often used as a gauge of a hospital’s overall efficiency (19). The three factors discussed above each contribute to reducing the average length of stay by reducing wastage, across lost time waiting (3), inefficient allocation of resources (9, 10), and misapplication of labour (15).
Shortening a patient's length of stay by a single day can meaningfully reduce care costs. Prolonged stays raise complication rates, strain bed occupancy, increase admission delays and waiting times, and fuel dissatisfaction that undermines confidence in hospital performance (19).
- The chest pain interventions using a common group chat for coordination reduced median LOS for those presentations from 4 days to 2.5 days (6)
- At the Wound Care Command Centre, the digital-first care model cut admissions and length of stay for chronic wound patients and saved the District millions of dollars. After deducting operational costs, service use fell significantly, indicating that substantial benefits accrue from reducing unnecessary hospital time for these patients (20).
- Per Li and colleagues, interoperability can shorten interhospital transfer throughput time by 12.0%, while also cutting 30‑day all‑cause readmissions by 3%, demonstrating a clear positive impact on patient outcomes (11). CSIRO figures from New South Wales advise that transferring patients accounts for 7.3% of patients overall. The rate increases where patients live more rurally, or where the clinical response is more acute or less common (22).
- In the oral cancer patient study, the series of small communication improvement projects sourced from the clinical teams delivered reduced LOS for admitted patients by more than 22%, from 4.90 to 3.80 days (3).
- Distractions and interruptions, such as those discussed in the Hart study (13), can be linked to a decrease in stress experienced, as well as objective performance and outcomes (21). Further, by reducing the wasted minutes identified in the Hart survey, up to an hour per day of clinician labour can be recaptured and directed to patient care, saving the provider money.
The opportunity in Ikonix UMS and Connect.
Few robust studies have quantified hospital inefficiencies, implemented a digital health solution, and measured the outcome in terms of Length of Stay. The wide variability in patient presentations, clinical requirements, and demographics, as well as differences across international systems, makes this nearly impossible.
By studying specific, measurable issues like those here, we can identify patterns of time lost, misallocated resources, and unnecessary processes, as well as numerous ways in which the ambiguity or sheer scale and complexity of hospital operations can undermine care coordination.
Ikonix Technology’s expertise has seen us deliver two relevant solutions into hospital environments:
- Our Message Integration Engine (MIE)—the core of the Ikonix UMS—to ingest data from systems or as triggered by personnel, and then broadcast it in line with customised workflows, and
- Ikonix Connect, a clinical messaging platform that receives alerts from systems and allows personnel to collaborate under healthcare-level security.
With a successful implementation of the MIE, clinical experiences such as interhospital transfers (11), surgery patient movement (7), imaging and radiology service utilisation (12), and pathology test ordering (9) would all be improved.
Further, a large rollout of Ikonix Connect would likely be able to achieve the required outcomes of reducing interruptions and distractions, and enabling clinicians to find the appropriate colleague faster (13), providing a collaboration environment as achieved for chest pain presentations (6), supporting the team and ward-level improvements of Lean (3) and support delivery of virtual clinic solutions similar to the Wound Care Command Centre (20).
Deploying these two interrelated services at a hospital would increase the time and resources available to patients. We estimate a conservative efficiency dividend of 5-10% across the entire hospital, based on the meta-assessment of the studies here.
Digital health solutions cannot necessarily affect the time it takes for patients to heal physically, but they can better control other variables. A 5% increase in productivity at the scale of a healthcare facility amounts to savings in the millions of dollars.

Your efficiency gains could eclipse the deployment cost.
Get in touch for a demo and learn where to target digital health solutions within your hospital:
References
- Australian Institute of Health and Welfare [AIHW] (2025) Health expenditure Australia 2023–24; [Open Link]
- Australian Medical Association (2025) Ambulance Ramping Report Card 2025 [Open Link]
- Fiorillo A, Sorrentino A, Scala A, Abbate V, Dell’Aversana Orabona G (2021) Improving performance of the hospitalisation process by applying the principles of lean thinking. TQM J. 2021;33(7):253-271. doi:10.1108/tqm09-2020-0207
- Health Performance Council (2025), ‘Room to improve patient flow, 2023-24 — Length of stay trends and variation across metropolitan Adelaide public acute hospitals, including comparisons of safety, quality and impact on emergency departments’, Government of South Australia. [Open Link]
- Zeiler, J., & Strazovska, L. (2025). Enhancing Hospital Efficiency in Germany: Process Management and Scheduling Innovations in Patient Logistics. Medical Perspectives / Medičnì Perspektivi, 30(4), 223–237. https://doi-org.rp.nla.gov.au/...
- Alhejily, WA (2021) Implementing “Chest Pain Pathway” Using Smartphone Messaging Application “WhatsApp” as a Corrective Action Plan to Improve Ischemia Time in “ST-Elevation Myocardial Infarction” in Primary PCI Capable Centre “WhatsApp-STEMI Trial”. Critical Pathways in Cardiology 20(4):p 179-184, December 2021. | DOI: 10.1097/HPC.0000000000000264
- Agency for Clinical Innovation (2026) Approaches to reduce surgical waiting time and waitlist: Living evidence, Critical Intelligence Unit, NSW Health [Open Link]
- Institute for Healthcare Improvement (2011) Innovation Series: Hospital Inpatient Waste Identification Tool; [Open Link]
- Brouillard, d, Pickavance, s, Hammoud, W (2025) Low Clinical Value Pathology Tests in the Emergency Department: Audit of Urine Microbiology and Culture Use at a Large Regional Centre, Emergency Medicine Australasia37, no. 6 (2025): e70162, https://doi.org/10.1111/1742-6....
- Krzywy, J, Dorofiejczuk, K, Młodawska, P, Jasiulewicz-Kaczmarek, M, & Nowak, F (2025). Mobile Solutions for Efficiency of Logistic Processes in Hospitals Improvement. LogForum, 21(2), 273–285. https://doi-org.rp.nla.gov.au/...
- Li, Y, Lu, LX, Lu, SF, & Chen, J (2022) The Value of Health Information Technology Interoperability: Evidence from Interhospital Transfer of Heart Attack Patients. Manufacturing & Service Operations Management (M&SOM), 24(2), 827–845. https://doi-org.rp.nla.gov.au/...
- Yahata, S, Tanaka, I, Takeuchi, M (2025) Development of a centralized progress management system using lean thinking and efforts to improve operations. BMC Health Serv Res 25, 1611 (2025). https://doi.org/10.1186/s12913...
- Hart, GK, Hosking, N, Martin, L & Todd, J (2025) Technology-based challenges of informal clinical communication in an Australian tertiary referral hospital: a survey-based assessment of user perspectives. BMJ Open Quality, 14(2). https://doi-org.rp.nla.gov.au/...
- Alexander, L, Moore, S, Salter, N, & Douglas, L (2020) Lean management in a liaison psychiatry department: implementation, benefits and pitfalls. BJPsych Bulletin, 44(1), 18–25. doi:10.1192/bjb.2019.64
- Cotton C, Mahut C, Blyth J, (2020) Using lean to improve wait time performance in diagnostic assessment for lung cancer. Healthc Q. 2020; 22(4):59-63. doi:10.12927/hcq.2020.26082
- Vijaykumar, A, Goodman, D, Whitcomb, R, Ruther, M, Miloshov, A, Pallini, M, Layton, J, O’Connor, D (2026) Reducing Postoperative Acute Kidney Injury: A Regional Quality Improvement Initiative of 26 Community-Based Hospitals, The Joint Commission Journal on Quality and Patient Safety, Volume 52, Issue 4, Pages 144-153, https://doi.org/10.1016/j.jcjq...
- Zhang Y, Zhu Y, Jiang T, Liu J, Tang X, Yi W (2023) An in-hospital stroke system to optimize emergency management of acute ischemic stroke by reducing door-to-needle time. Am J Emerg Med. 2023 Jul;69:147-153. doi: 10.1016/j.ajem.2023.04.008. Epub 2023 Apr 11. PMID: 37119700
- Isaacs, AN, & Duncan, Z (2025) Care coordination for persons with mental health challenges: a scoping review. International Journal of Mental Health Systems, 19(1), 1–16. https://doi-org.rp.nla.gov.au/...
- Kulkarni, M, & Dongre, P (2023) Determining Efficacy of Inpatient Care for Select Surgeries at a Large Tertiary Care Hospital With Average Length of Stay as a Measure. Hospital Topics, 101(1), 48–53. https://doi-org.rp.nla.gov.au/... [Open Link]
- Barakat-Johnson, M, Newton, M, Cayley, C, Lai, M, Dixie, L, Alexander, N, Pelusi, M, Chan, J, & Cohen, A (2025) Digitising wound care: a cost-consequence analysis of the Wound Care Command Centre™ in Australia. BMC Health Services Research, 25(1), 1–15. https://doi-org.rp.nla.gov.au/...
- Mackenzie & Foran (2020) The impact of distractions and interruptions in the operating room on patient safety and the operating room team: An integrative review; Journal of Perioperative Nursing Volume 33 Number 3 Spring 2020
- Assareh, H, Achat, H, Levesque, J, Leeder, S (2017) Exploring interhospital transfers and partnerships in the hospital sector in New South Wales, Australia, Aust Health Rev (2017) 41 (6): 672–679, https://doi.org/10.1071/AH1611...